The first time the team had seen the entire scheduling system laid out in one place.
The symptoms were visible. The cause took real digging to find.
On the surface, the complaints were straightforward: clinicians were missing appointments, booking conflicts were frequent, and patients were churning. But the pain points weren't pointing to a design problem. They were pointing to something structural.
And critically, none of this was integrated with the EMR where clinicians actually did their work. Almost nobody on the team fully understood how the scheduling architecture had been built or why. One engineer held most of that institutional knowledge. I worked closely with him to reconstruct the history of the system and understand the constraints we were actually working within.
Before I could design anything, I had to make the problem visible to the whole team.
I led clinician interviews, shadowing sessions, and stakeholder workshops to understand how scheduling actually worked in practice. What I found confirmed the structural diagnosis: clinicians were regularly working around the system rather than through it, and the workarounds were generating their own errors.
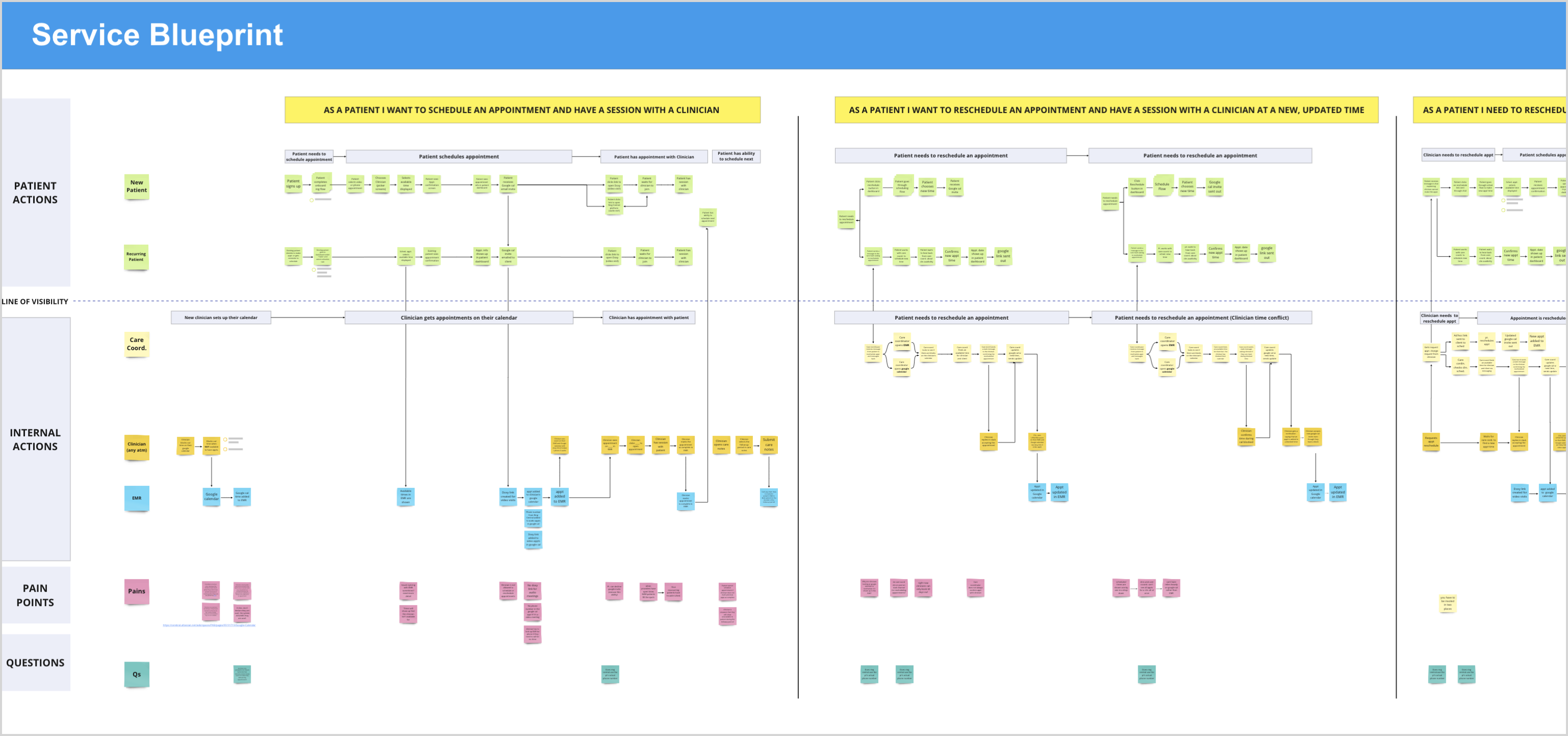
The most important artifact I built wasn't a wireframe. It was a service blueprint mapping the full scheduling and availability process across every touchpoint. It was the first time anyone on the team had seen the entire system laid out in one place.
That blueprint became the primary tool for getting alignment. It made visible what had previously been fragmented institutional knowledge, and gave the team a shared language for what was broken and why.
After research, the direction was clear: the scheduling system needed to move inside the EMR. As long as it lived outside, clinicians would be context switching between two systems, availability data would stay out of sync, and the underlying source of booking conflicts would remain untouched.
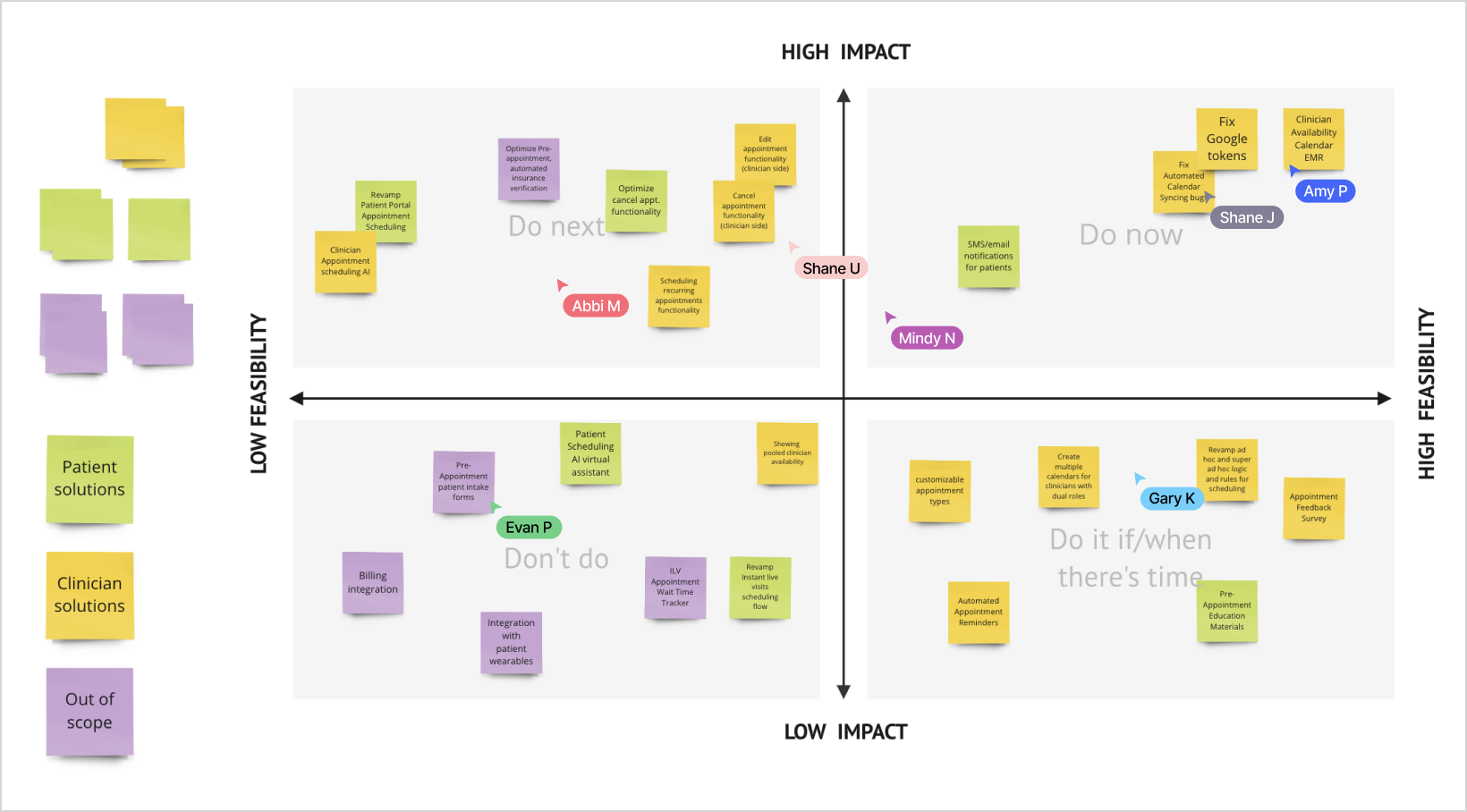
But integration was significant engineering work. I facilitated a priority matrix workshop with the full team, mapping potential solutions by impact and feasibility. It gave us a structured way to have an honest conversation about what to pursue now, what to defer, and what to take off the table entirely.
The outcome shaped the MVP scope: integrate availability and appointment management directly into the EMR. Recurring and multiple appointment flows were scoped explicitly as a next phase, not cut from the vision.
The design work was about collapsing two fragmented systems into one coherent experience.
I guided the design phase in close collaboration with the designer on the project, providing direction, feedback, and hands-on support as needed. We partnered with engineering throughout to ensure the new features could be implemented within the existing system architecture.
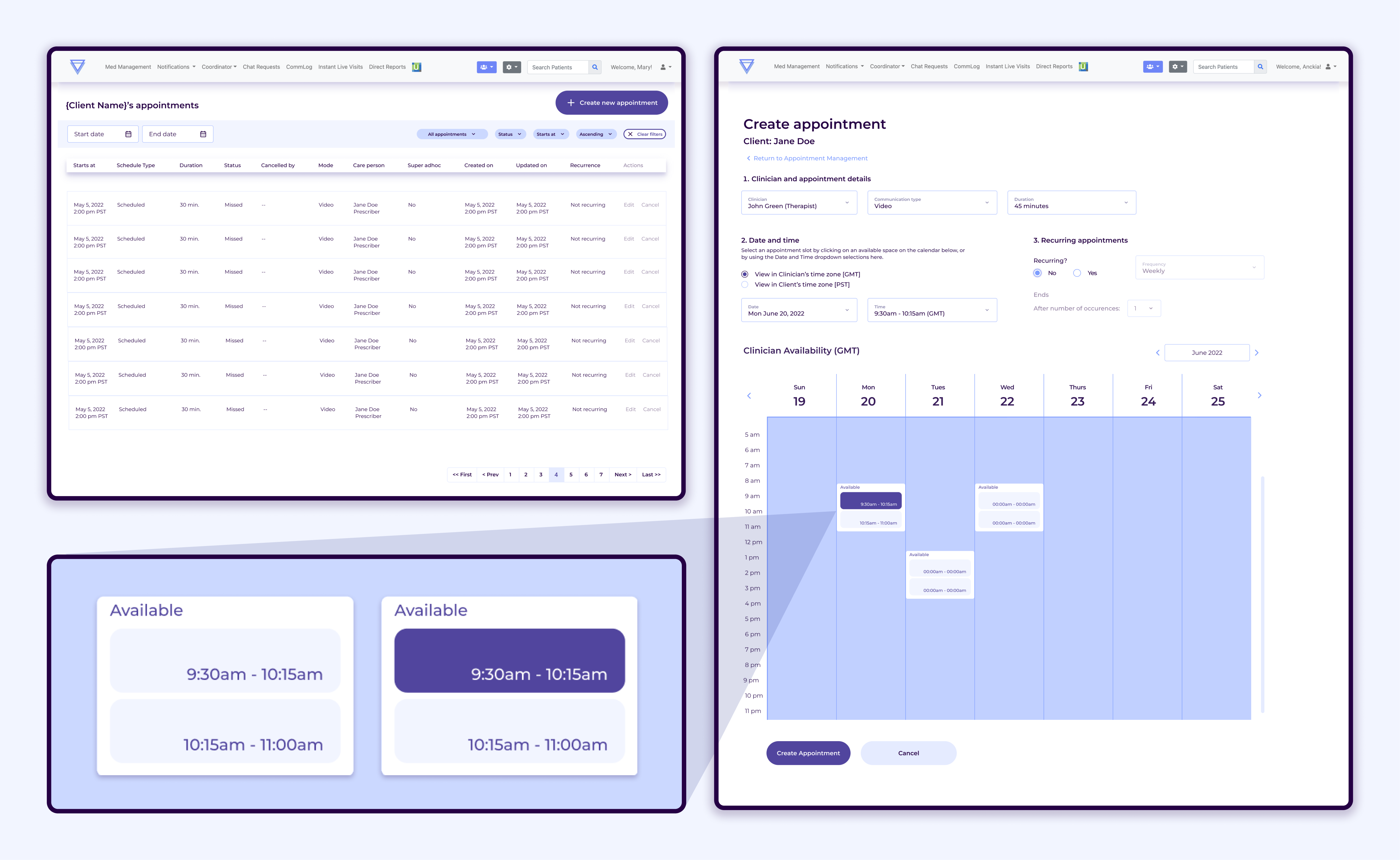
The core of the new experience was a clinician availability calendar built directly into the EMR. Clinicians could now mark availability positively, view their schedule in the same context as their patient records, and see appointment slots in real time alongside care team members coordinating bookings.
What shipped was a foundation. What it replaced was a chronic source of operational failure.
The integrated scheduling system gave clinicians and care team members something the previous setup couldn't: a single, reliable place to understand availability, coordinate appointments, and avoid conflicts. The structural cause of the double bookings and missed sessions was addressed at the root rather than patched at the surface.
Recurring and multiple appointment functionality was scoped and documented for the next phase. The groundwork was in place to build on.
This project required more than design. It required reconstructing institutional knowledge, translating a fragmented system into something the team could reason about together, and advocating for an approach that was harder to build but right for the long term. That's the work that made the design work possible.
